NStarX – From Hospital Beds to Studio Sets: Applying Healthcare’s Predictive Census AI to Media Workforce Optimization
Sujay Kumar(CRO), Suman Kalyan (CAIO), NStarX Inc.
Why Healthcare’s Predictive Census AI Maps Directly to Media Production
Both healthcare and media production face the same operational challenge: managing a large, specialized workforce under volatile, high-stakes demand. In hospitals, patient inflow unpredictability strains staffing, while in media production, fluctuating project pipelines drive overtime, budget overruns, and resource conflicts. Healthcare has already solved this problem at scale using predictive census AI—forecasting demand with >90% accuracy and optimizing staffing in real time. Media production follows a structurally similar pattern: patient flow mirrors project flow, departments mirror production units, and clinical resources map to crew, studios, and equipment. By adapting healthcare’s proven architecture—time-series forecasting, ensemble models, and visual operational dashboards—media companies can shift from reactive scheduling to proactive workforce management, unlocking significant reductions in overtime, idle time, and budget variance.
The Costly Challenge of Workforce Mismanagement
Human capital represents the largest operational expense in both healthcare and media production, yet effective resource allocation remains elusive. In healthcare, the financial toll is staggering: hospital labor costs surged 258% between 2019-2022, with staffing shortages costing $24 billion in 2021, projected to reach $86 billion by year’s end. Contract labor expenses skyrocketed 257.9%, while median wages to staffing firms rose 56.8%. Each registered nurse vacancy costs approximately $175,000 annually at medium-sized hospitals, while emergency departments experienced 22% more overtime hours per visit.
Media production faces parallel challenges. Film productions routinely exceed budgets by 31%, with independent films overshooting by 40%. Workforce costs consume 30-40% of total budgets. Notable examples: ‘Cleopatra’ (1963) ballooned from $2 million to $44 million (equivalent to $340 million today), while ‘Waterworld’ (1995) escalated from $100 million to $175 million, both partially due to crew management failures. Coordinating specialized talent across production phases, managing union requirements, and controlling overtime creates persistent margin erosion.
Healthcare’s AI-Powered Breakthrough
Healthcare organizations have turned to artificial intelligence and machine learning for workforce optimization, with 65% of U.S. hospitals now deploying AI-assisted predictive models. These solutions leverage sophisticated time-series forecasting architectures, with Long Short-Term Memory (LSTM) networks and Gated Recurrent Units (GRUs) emerging as preferred models for capturing temporal dependencies in sequential healthcare data. LSTM-based models achieve remarkable accuracy levels of 92.4% with 90.1% precision in predicting patient outcomes and resource
needs. Ensemble approaches combining ARIMA (statistical time-series models), multilayer perceptrons, and LSTM networks deliver even superior performance, with relative 95% confidence intervals of ±3.4% for 12-hour census predictions.
The implementation architecture typically includes data ingestion layers pulling from Electronic Health Record (EHR) systems, preprocessing pipelines handling irregular time-series data and missing values, and real-time dashboard applications delivering actionable insights to hospital administrators. Hawaii Pacific Health exemplifies successful deployment, using predictive analytics for workforce forecasting and scheduling to transition from retrospective planning to proactive management, achieving 10-20% improvements in staff utilization and 15% reductions in overtime and agency labor costs. The system analyzes historical admission data, patient trends, seasonality, and real-time variables to ensure right-sized staffing at optimal times.
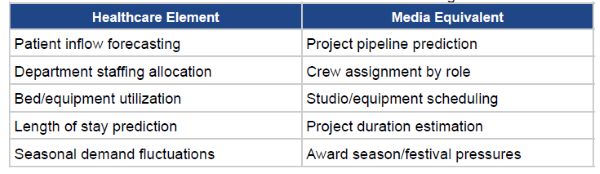
Healthcare-Media Workforce Parallels
While healthcare provides rich quantitative insights into workforce strain, media production exhibits the same pattern in financial and operational terms. Hospitals face cost inflation through overtime and contract labor; media productions experience parallel erosion through union overtime rates, freelancer premiums, schedule delays, and department overruns. The numerical symmetry is striking: healthcare sees 10–20% workforce inefficiency, while films exceed budgets by 31–40%—a function of the same underlying failure to predict demand and align labor in advance. This structural alignment strengthens the case for transferring predictive census AI from healthcare to media with minimal architectural change.
Translating Healthcare’s AI Architecture
Healthcare’s proven architecture translates directly to media with minimal modification. Core components—time-series forecasting engines, ensemble ML models, and operational dashboards—remain consistent. The data layer integrates production management systems, casting databases, equipment platforms, and historical project data. LSTM/GRU networks learn from project types, crew requirements, equipment dependencies, and seasonal cycles.
The prediction engine forecasts project demand, optimal crew allocation, resource conflicts, and budget risks. Dashboards provide production managers with staffing recommendations, equipment optimization, overtime alerts, and conflict warnings. While tools like Filmustage and Autodesk Flow have begun incorporating scheduling capabilities, comprehensive predictive census functionality remains nascent.
Simplified Three-Layer Architecture for Executives
To make the AI approach intuitive for production leaders, the full technical architecture can be summarized in three simple layers:
• Data Layer – Ingests project schedules, casting data, equipment inventories, historical productions, and union rules into a unified data lake.
• Intelligence Layer – Uses LSTM/GRU models, ARIMA ensembles, and attention mechanisms to forecast project demand, staffing levels, equipment conflicts, and overtime risk.
• Action Layer – Delivers clear recommendations through dashboards: optimal crew allocation, resource heatmaps, overtime warnings, budget variance predictions, and automated scheduling.
This streamlined view gives executives immediate clarity on how predictive census AI transforms production planning from reactive firefighting to proactive resource orchestration.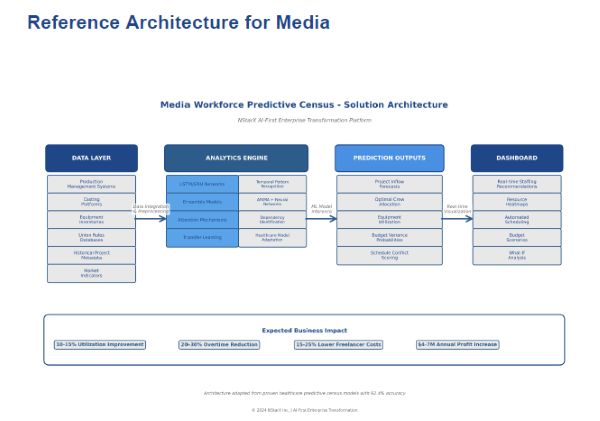
Figure 1: Media Workforce Predictive Census- Solution Architecture
Data Layer: Production systems, casting platforms, equipment inventories, union rules, historical project metadata, market indicators.
Analytics Engine: LSTM/GRU networks for temporal patterns, ensemble models combining ARIMA with neural networks, attention mechanisms for dependencies, transfer learning from healthcare.
Prediction Outputs: Project inflow forecasts, optimal crew allocation, equipment utilization, budget variance probabilities, schedule conflict scoring.
Dashboard: Real-time staffing recommendations, resource heatmaps, automated scheduling, budget scenarios, what-if analysis.
Revenue Impact
Predictive census offers multiple revenue pathways. Direct cost savings: 10-15% reductions in idle time, 20-30% decreases in overtime, 15-25% lower freelancer premiums. Enhanced throughput enables more concurrent projects without proportional cost increases, while faster completion accelerates revenue recognition. Accurate bid pricing improves win rates and margins.
Strategic capacity planning unlocks new revenue streams through proactive capacity investments aligned with forecasted demand. For mid-sized production companies processing $50M revenue annually, conservative 8-12% utilization improvements and 5-7% throughput increases could generate $4-7M additional annual profit.
Implementation Challenges
Successful deployment requires overcoming three critical challenges:
• Data Fragmentation – Media lacks an integrated equivalent to healthcare’s EHR systems. Solving this requires consolidating scheduling tools, budgeting software, and equipment platforms into a single governed data layer.
• High Creative Variability – Unlike standardized clinical pathways, productions range dramatically by genre, budget, director style, and VFX intensity. This is mitigated through ensemble modeling, project taxonomies, and complexity-weighted feature engineering.
• Cultural Resistance – Production teams may perceive AI recommendations as limiting creative autonomy. Adoption improves when AI is framed as augmentation—not replacement—and introduced through transparent pilot programs.
These streamlined challenges make the path to implementation clearer for executive decision-makers.
Conclusion
Healthcare’s success with predictive census AI demonstrates that workforce optimization in complex, high-variability environments is not only possible—it is proven. Media production mirrors healthcare’s operational structure: unpredictable demand, high labor intensity, expensive overtime, and cascading resource dependencies. By applying the same predictive architecture, media companies can achieve measurable gains: 20–30% reduction in overtime, 10–15% reduction in idle crew time, 15–25% lower freelancer premiums, and 5–7% higher throughput without increasing headcount. In an industry where margins are tightening and project complexity is rising, predictive workforce optimization is no longer a future ambition—it is a strategic imperative for competitiveness, profitability, and sustainable growth. The technology is validated, the architecture transferable, and the financial upside compelling.
References
1. Healthcare Finance News (2023). ‘Hospitals’ labor costs increased 258% over the last three years.’
2. American Hospital Association (2021). ‘Health Care Workforce Challenges.’
3. Filmustage (2024). ‘Film Budget Breakdown by Department.’
4. Health Affairs (2024). ‘AI and Predictive Models In US Hospitals.’
5. PMC (2020). ’12-hour hospital census prediction algorithm.’ NIH.
6. ACM Transactions (2022). ‘Time Series Prediction Using Deep Learning in Healthcare.’
7. Frontiers (2020). ‘AI in Healthcare: Time-Series Forecasting Architectures.’